















 19 / 36
19 / 36

CAMLOG&Science – Chapter 3
18 | 19
RETRIEVABILITY OF CEMENT-RETAINED IMPLANT CROWNS
Cement-retained restorations are regarded to have advantages when com-
pared to screw-retained restorations since they allow improved esthetics and
eliminate the risk of screw loosening. However, restorations may need to be re-
trieved in case of technical or biological complications. Mehl et al. (2012a and
2012b) compared in their in vitro studies different cement-retained materials
regarding strength and crown retrievability. Crowns which were cement-
retained to CAMLOG
®
titanium abutments using a glass-ionomer cement
could significantly easier be removed than crowns cement-retained with a poly-
carboxylate or with resin cement. The authors concluded that glass-ionomer
cement can serve as a semipermanent solution while polycarboxylate or com-
posite resin cements should be used for permanent cementations.
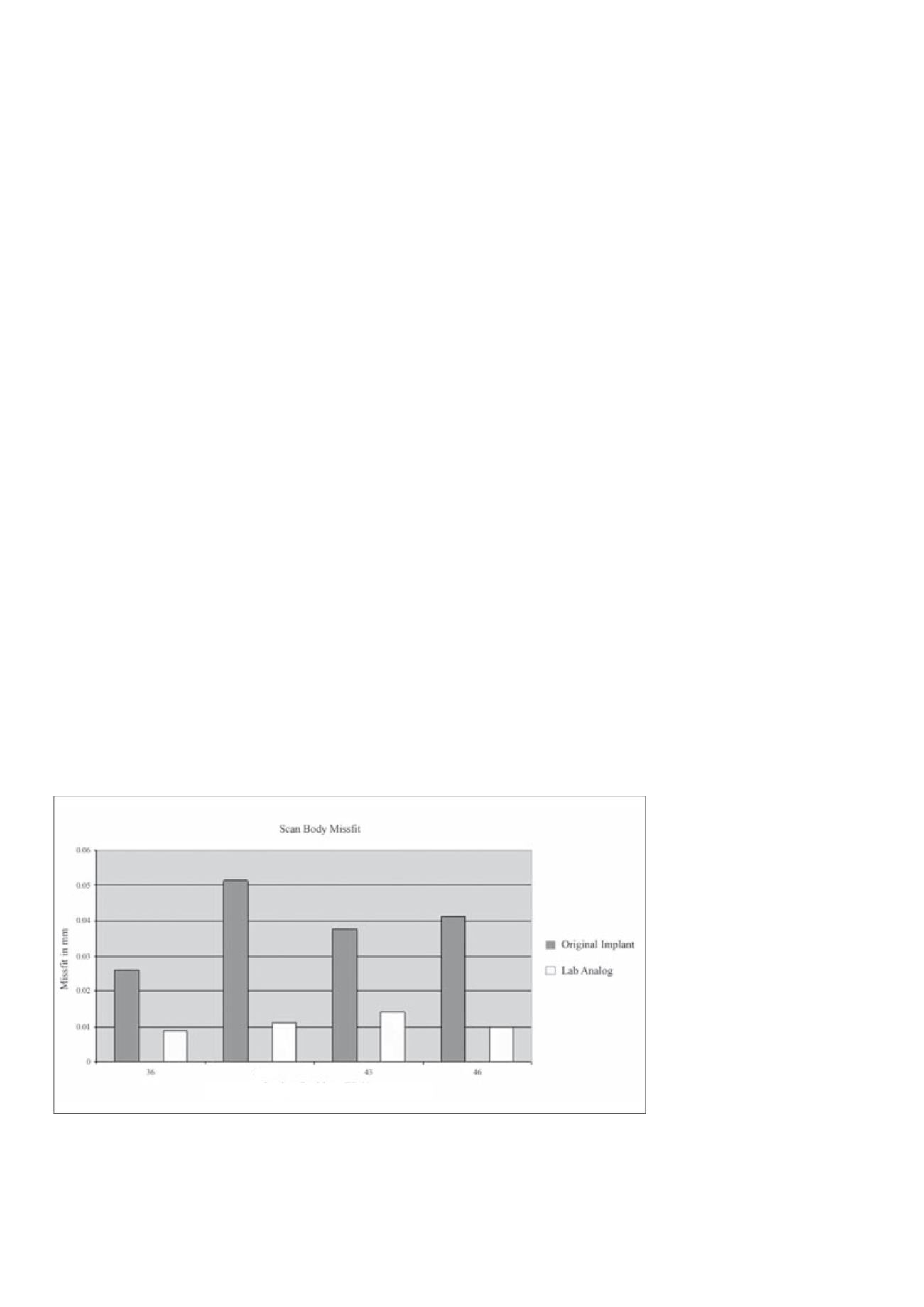
Fig. 13:
The mean discrepancies of the scanbodies at the different implant sites (FDI 36, 33, 43,
and 46) for the original implants and the lab analogues are shown (Stimmelmayr et al., 2012c
reproduced with kind permission of Springer).
PASSIVE FIT OF PROSTHETICS: IMPRESSION TECHNIQUES AND
REPRODUCIBILITY OF SCANBODY FIT
Passive fit of prosthodontics is only achieved when the accuracy of the implant
transfer between the original situation and the cast is optimal. Stimmelmayr
et al. (2012b) digitally compared the accuracy of different impression tech-
niques, i.e., transfer, pick-up and splinted pick-up. They inserted CAMLOG
®
SCREW-LINE implants into lower-arch models and took impressions. Scan-
bodies were mounted on the implants of the original models and on the lab
analogues of stone casts and were digitized. Discrepancy between original
and cast was 124 ± 34 μm for the transfer technique and 116 ± 46 μm for
the pick-up technique. Least discrepancy was found for the splinted pick-up
technique (80 ± 25 μm). The authors concluded that the splinted pick-up
technique is recommendable for impressions when placing four implants
evenly distributed in the edentulous jaw.
In their second study, the researchers evaluated the reproducibility of the
scanbody fit (Stimmelmayr et al. 2012c). Scans were taken before and after
repeatedly removing and re-attaching scanbodies to the same implant on
the original model or to the lab analogue on stone casts. Comparison of
these scans revealed a mean scanbody discrepancy of 39 ± 58 μm on origi-
nal implants. Discrepancy of scanbodies on the lab analogues was signifi-
cantly lower (mean 11 ± 17 μm) indicating a better reproducibility of the
scanbody position (Fig. 13). The authors emphasized the importance of low
manufacturing tolerances.
33
Implant Position (FDA)